| Symptome associé : | | |
| La douleur pelvienne chronique au cours du cycle menstruel est souvent associée à une dysménorrhée
Dysménorrhée .. cacher .... voir plus ..
La dysménorrhée peut être classée primaire ou secondaire en fonction de l'absence ou de la présence d'une cause sous-jacente. La dysménorrhée secondaire est une dysménorrhée associée à une affection existante.
Le recueil des antécédents et un examen clinique, y compris un examen pelvien, peuvent révéler la cause.
Les saignements utérins anormaux, la dyspareunie, les douleurs non cycliques, les changements d'intensité et la durée de la douleur, et les résultats anormaux d'examen pelvien suggèrent une pathologie sous-jacente (dysménorrhée secondaire) et nécessitent une recherche plus approfondie.
La cause la plus fréquente de dysménorrhée secondaire est l'endométriose.
D'autres causes de dysménorrhée secondaire comprennent les fibromes utérins, l'adénomyose, les kystes ovariens, les anomalies de Mullerian, les adhérences pelviennes et la congestion pelvienne.
... lire plus sur ce sujet dans un nouvel onglet.... |  | |
| Anomalie ou Maladie évoquée : | | |
| La douleur pelvienne qui varie considérablement au cours du cycle menstruel est probablement attribuable à une affection hormonale telle que l'endométriose.
Endométriose .. cacher .... voir plus ..
L'endométriose désigne une affection se caractérisant par une implantation du tissu endométrial dans des localisations autres que celle de la muqueuse utérine.
L'endométriose est retrouvée de manière prédominante au niveau du colon sigmoïde, du rectum antérieur, de l'iléon terminal et du caecum.
Ce qui demeure frappant est la quasi absence de développement du tissu endométrial dans les trompes de Fallope. De nombreuses autres localisations peuvent être retrouvées.
Considérée comme une tumeur bénigne, il a été toutefois rapporté des cas de malignité.
L'endométriose est une maladie chirurgicale. Le traitement médical (danazol, leucoprolide, contraceptifs oraux) ne permet qu'un soulagement temporaire de la douleur, mais aucun traitement médical n'a été efficace dans le traitement de l'endométriose. Seule une prise en charge chirurgicale est efficace et permet d'éradiquer la maladie.
... lire plus sur ce sujet dans un nouvel onglet.... | 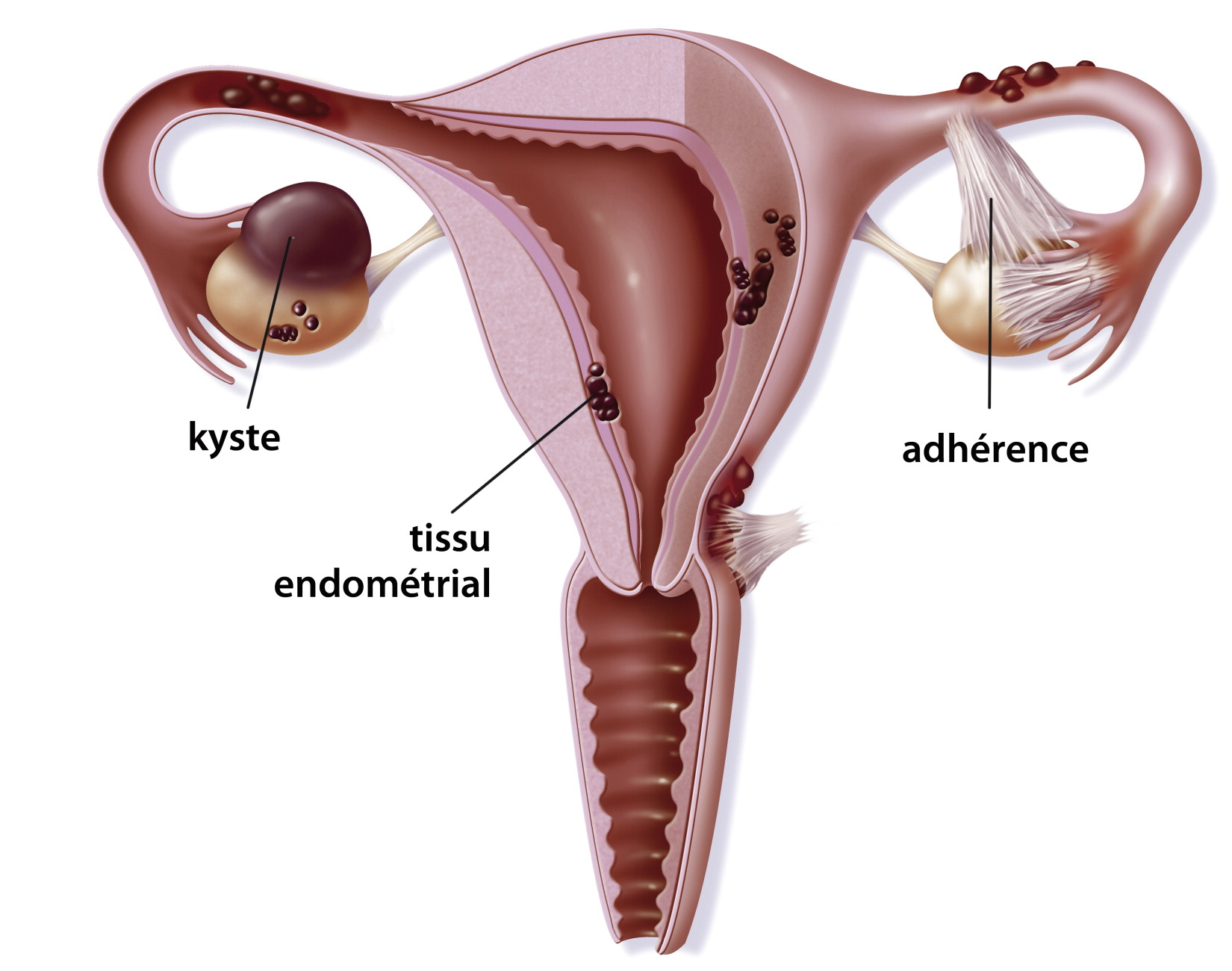 | |
| Douleur légère et récurrente dans le bas-ventre
Maladie inflammatoire pelvienne (MIP) .. cacher .... voir plus ..
La maladie inflammatoire pelvienne (MIP) chronique est la principale cause de l'infertilité tubulaires et constitue un facteur de risque important de grossesse extra-utérine.
Le MIP chronique est accompagné des signes et symptômes suivants: Douleur légère et récurrente dans le bas-ventre; Mal au dos; règles irrégulières; Douleur pendant les rapports sexuels; Infertilité; pertes vaginale importanteset désagréable.
Le risque de MIP augmente à la suite d'épisodes répétés de MIP aigu (résultats d'une infection sexuellement transmissible, comme la chlamydia ou la gonorrhée, les personnes atteintes de MIP peuvent ne pas avoir de symptômes. Lorsque les symptômes se produisent, ils peuvent être non spécifiques, comme les douleurs abdominales, une fièvre élevée et des vomissements).
... lire plus sur ce sujet dans un nouvel onglet.... |  | |
| Adhérences pelviennes .. cacher .... voir plus ..
Les adhérences pelviennes sont des tissus ou des cicatrices fibreuses qui se développent dans la cavité pelvienne entre l'utérus, les trompes de Fallope, les intestins et la vessie.
En outre, ils peuvent être trouvés à l'intérieur des trompes et de l'utérus. Ces adhérences peuvent bloquer ou tordre les trompes de Fallope.
Il existe 3 causes principales d'adhésions pelviennes et de lésions tubaires:
. Infections pelviennes
. Traumatismes chirurgicaux
. Endométriose
... lire plus sur ce sujet dans un nouvel onglet.... | 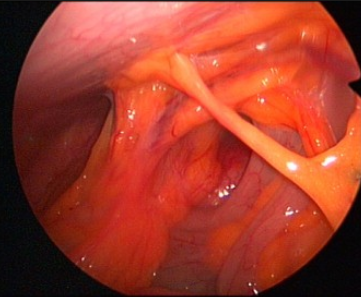 | |
| Cervicite .. cacher .... voir plus ..
La cervicite est une inflammation cervicale aiguë ou chronique;
elle peut être infectieuse ou non infectieuse.
La cervicite se présente le plus souvent sous forme de pertes vaginales ou de saignement postcoital
Etiologie: Souvent, aucune etiologie spécifique n'est identifiée.
Infectieux: Chlamydia trachomatis et Neisseria gonorrhoeae sont les agents pathogènes les plus fréquemment identifiés; ils affectent l'épithélium colonnaire de l'endocervix. Trichomonas vaginalis, HSV (en particulier les infections primaires du HSV-2) et le HPV affectent l'épithélium squameux.
Les mycoplasmes (par exemple, Mycoplasma genitalium) sont de plus en plus reconnus comme un organisme causal.
Non infectieux: irritation physique ou chimique (par exemple, douches douces, exposition au latex, crèmes contraceptives ou corps étrangers vaginaux tels que tampons, capsules cervicales), radiothérapie, maladies inflammatoires, malignité
... lire plus sur ce sujet dans un nouvel onglet.... |  | |
| Kyste folliculaire persistant fonctionnel ou organique .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... |  | |
| Kyste lutéinique : follicule lutéinisé non rompu .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... |  | |
| Divers | | |
| De nombreuses femmes décrivent des douleurs en début de grossesse.
En général, ces douleurs temporaires, ne sont pas inquiétantes.
Bien que pouvant être liées à un kyste ovarien ou à une constipation, elles peuvent aussi être:
* un signe précoce de grossesse extra-utérine et alors une urgence
* ou indiquer l'existence d'une problème important tel qu'une lithiase rénale.
Autre, divers: Début de grossesse .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Référence : | | |
| Pain typology and incident endometriosis .. cacher .... voir plus ..
STUDY QUESTION What are the pain characteristics among women, with no prior endometriosis diagnosis, undergoing laparoscopy or laparotomy regardless of clinical indication? SUMMARY ANSWER Women with surgically visualized endometriosis reported the highest chronic/cyclic pain and significantly greater dyspareunia, dysmenorrhea, and dyschezia compared with women with other gynecologic pathology (including uterine fibroids, pelvic adhesions, benign ovarian cysts, neoplasms and congenital Müllerian anomalies) or a normal pelvis. WHAT IS KNOWN ALREADY Prior research has shown that various treatments for pain associated with endometriosis can be effective, making identification of specific pain characteristics in relation to endometriosis necessary for informing disease diagnosis and management. STUDY DESIGN, SIZE, DURATION The study population for these analyses includes the ENDO Study (2007–2009) operative cohort: 473 women, ages 18–44 years, who underwent a diagnostic and/or therapeutic laparoscopy or laparotomy at one of 14 surgical centers located in Salt Lake City, UT or San Francisco, CA. Women with a history of surgically confirmed endometriosis were excluded. PARTICIPANTS/MATERIALS, SETTING AND METHODS Endometriosis was defined as surgically visualized disease; staging was based on revised American Society for Reproductive Medicine (rASRM) criteria. All women completed a computer-assisted personal interview at baseline specifying 17 types of pain (rating severity via 11-point visual analog scale) and identifying any of 35 perineal and 60 full-body front and 60 full-body back sites for which they experienced pain in the last 6 months. MAIN RESULTS AND THE ROLE OF CHANCE There was a high prevalence (≥30%) of chronic and cyclic pelvic pain reported by the entire study cohort regardless of post-operative diagnosis. However, women with a post-operative endometriosis diagnosis, compared with women diagnosed with other gynecologic disorders or a normal pelvis, reported more cyclic pelvic pain (49.5% versus 31.0% and 33.1%, P < 0.001). Additionally, women with endometriosis compared with women with a normal pelvis experienced more chronic pain (44.2 versus 30.2%, P = 0.04). Deep pain with intercourse, cramping with periods, and pain with bowel elimination were much more likely reported in women with versus without endometriosis (all P < 0.002). A higher percentage of women diagnosed with endometriosis compared with women with a normal pelvis reported vaginal (22.6 versus 10.3%, P < 0.01), right labial (18.4 versus 8.1%, P < 0.05) and left labial pain (15.3 versus 3.7%, P < 0.01) along with pain in the right/left hypogastric and umbilical abdominopelvic regions (P < 0.05 for all). Among women with endometriosis, no clear and consistent patterns emerged regarding pain characteristics and endometriosis staging or anatomic location. LIMITATIONS, REASONS FOR CAUTION Interpretation of our findings requires caution given that we were limited in our assessment of pain characteristics by endometriosis staging and anatomic location due to the majority of women having minimal (stage I) disease (56%) and lesions in peritoneum-only location (51%). Significance tests for pain topology related to gynecologic pathology were not corrected for multiple comparisons. WIDER IMPLICATIONS OF THE FINDINGS Results of our research suggest that while women with endometriosis appear to have higher pelvic pain, particularly dyspareunia, dysmenorrhea, dyschezia and pain in the vaginal and abdominopelvic area than women with other gynecologic disorders or a normal pelvis, pelvic pain is commonly reported among women undergoing laparoscopy, even among women with no identified gynecologic pathology. Future research should explore causes of pelvic pain among women who seek out gynecologic care but with no apparent gynecologic pathology. Given our and other s research showing little correlation between pelvic pain and rASRM staging among women with endometriosis, further development and use of a classification system that can better predict outcomes for endometriosis patients with pelvic pain for both surgical and nonsurgical treatment is needed. STUDY FUNDING/COMPETING INTERESTS Supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development (contracts NO1-DK-6-3428, NO1-DK-6-3427, and 10001406-02). The authors have no potential competing interests.
... lire plus sur ce sujet dans un nouvel onglet.... | | |  |
| Progestagens and anti-progestagens for pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is a chronic inflammatory condition defined by the presence of glands and stroma outside the uterine cavity. It occurs in 7% to 10% of all women of reproductive age and may present as pain or infertility. The pelvic pain may be in the form of dysmenorrhoea, dyspareunia or pelvic pain. Initially a combination of estrogens and progestagens was used to create a pseudopregnancy and alleviate the symptoms associated with endometriosis. Progestagens alone or anti-progestagens have been considered as alternatives because they are inexpensive and may have a better side effect profile than other choices. Objectives Objectives To determine the effectiveness of both the progestagens and anti-progestagens in the treatment of painful symptoms ascribed to the diagnosis of endometriosis. Search methods Search methods We used the search strategy of the Menstrual Disorders and Subfertility Group to identify all publications which described or might have described randomised controlled trials (RCTs) of any progestagen or any anti-progestagen in the treatment of symptomatic endometriosis. We updated the review in 2011. Selection criteria Selection criteria We considered only RCTs which compared the use of progestagens and anti-progestagens with other interventions, placebo or no treatment for the alleviation of symptomatic endometriosis. Data collection and analysis Data collection and analysis We have added six new studies, bringing the total of included studies to 13 in the update of this review. The six newly included studies evaluated progestagens (comparisons with placebo, danazol, oral or subdermal contraceptive, oral contraceptive pill and danazol, gonadotrophin-releasing hormone (GnRH) analogue and other drugs). The remaining studies compared the anti-progestagen gestrinone with danazol, GnRH analogues or itself. Main results Main results The progestagen medroxyprogesterone acetate (100 mg daily) appeared to be more effective at reducing all symptoms up to 12 months of follow-up (MD -0.70, 95% CI -8.61 to -5.39; P < 0.00001) compared with placebo. There was evidence of significantly more cases of acne (six versus one) and oedema (11 versus one) in the medroxyprogesterone acetate group compared with placebo. There was no evidence of a difference in objective efficacy between dydrogesterone and placebo. There was no evidence of a benefit with depot administration of progestagens versus other treatments (low dose oral contraceptive or leuprolide acetate) for reduced symptoms. The depot progestagen group experienced significantly more adverse effects. There was no overall evidence of a benefit of oral progestagens over other medical treatment at six months of follow-up for self-reported efficacy. Amenorrhoea and bleeding were more frequently reported in the progestagen group compared with other treatment groups. There was no evidence of a benefit of anti-progestagens (gestrinone) compared with danazol. GnRH analogue (leuprorelin) was found to significantly improve dysmenorrhoea compared with gestrinone (MD 0.82, 95% CI 0.15 to 1.49; P = 0.02) although it was also associated with increased hot flushes (OR 0.20, 95% CI 0.06 to -0.63; P = 0.006). Authors conclusions Authors conclusions There is only limited evidence to support the use of progestagens and anti-progestagens for pain associated with endometriosis.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Gonadotrophin-releasing hormone analogues for pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is a common gynaecological condition, characterised by the presence of endometrial tissue in sites other than the uterine cavity (excluding adenomyosis) that frequently presents with pain. The gonadotrophin-releasing hormone analogues (GnRHas) comprise one intervention that has been offered for pain relief in pre-menopausal women. GnRHas can be administered intranasally, by subcutaneous, or intramuscular injection. They are thought to result in down regulation of the pituitary and induce a hypogonadotrophic hypogonadal state. Objectives Objectives To determine the effectiveness and safety of GnRHas in the treatment of the painful symptoms associated with endometriosis. Search methods Search methods Electronic searches of the Cochrane Menstrual Disorders and Subfertility Group specialist register, CENTRAL, MEDLINE, EMBASE, PSYCInfo and CINAHL were conducted in April 2010 to identify relevant randomised controlled trials (RCTs). Selection criteria Selection criteria RCTs of GnRHas as treatment for pain associated with endometriosis versus no treatment, placebo, danazol, intra-uterine progestagens, or other GnRHas were included. Trials using add-back therapy, oral contraceptives, surgical intervention, GnRH antagonists or complementary therapies were excluded. Data collection and analysis Data collection and analysis Quality assessment and data extraction were performed independently by two reviewers. The primary outcome was pain relief. Relative risk was used as the measure of effect for dichotomous data. For continuous data, mean differences or standardised mean differences were used. Main results Main results Forty one trials (n=4935 women) were included. The evidence suggested that GnRHas were more effective at symptom relief than no treatment/placebo. There was no statistically significant difference between GnRHas and danazol for dysmenorrhoea RR 0.98 (95%CI 0.92 to 1.04; P = 0.53). This equates to 3 fewer women per 1000 (95%CI 12 to 6) with symptomatic pain relief in the GnRHa group. More adverse events were reported in the GnRHa group. There was a benefit in overall resolution for GnRHas RR1.10 (95%CI 1.01 to 1.21, P=0.03) compared with danazol. There was no statistically significant difference in overall pain between GnRHas and levonorgestrel SMD -0.25 (95%CI -0.60 to 0.10, P=0.46). Evidence was limited on optimal dosage or duration of treatment for GnRHas. No route of administration appeared superior to another. Authors conclusions Authors conclusions GnRHas appear to be more effective at relieving pain associated with endometriosis than no treatment/placebo. There was no evidence of a difference in pain relief between GnRHas and danazol although more adverse events reported in the GnRHa groups. There was no evidence of a difference in pain relief between GnRHas and levonorgestrel and no studies compared GnRHas with analgesics.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Danazol for pelvic pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is defined as the presence of endometrial tissue (stromal and glandular) outside the normal uterine cavity. Conventional medical and surgical treatments for endometriosis aim to remove or decrease the deposits of ectopic endometrium. The observation that hyper androgenic states (an excess of male hormone) induce atrophy of the endometrium has led to the use of androgens in the treatment of endometriosis. Danazol is one of these treatments. The efficacy of danazol is based on its ability to produce a high androgen and low oestrogen environment (a pseudo menopause) which results in atrophy of the endometriotic implants and thus an improvement in painful symptoms. Objectives Objectives To determine the effectiveness of danazol compared to placebo or no treatment in the treatment of the symptoms and signs, other than infertility, of endometriosis in women of reproductive age. Search methods Search methods We searched the Cochrane Menstrual Disorders and Subfertility Group Specialised Register of trials (searched April 2007), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 2, 2007), and MEDLINE (1966 to April 2007). In addition, all reference lists of included trials were searched, and relevant drug companies were contacted for details of unpublished trials. Selection criteria Selection criteria Randomised controlled trials in which danazol (alone or as adjunctive therapy) was compared to placebo or no therapy. Trials which only reported infertility outcomes were excluded. Data collection and analysis Data collection and analysis Only five trials met the inclusion criteria and two authors independently extracted data from these trials. All trials compared danazol to placebo. Three trials used danazol as sole therapy and three trials used danazol as an adjunct to surgery. Although the main outcome was pain improvement other data relating to laparoscopic scores and hormonal parameters were also collected. Main results Main results Treatment with danazol (including adjunctive to surgical therapy) was effective in relieving painful symptoms related to endometriosis when compared to placebo. Laparoscopic scores were improved with danazol treatment (including as adjunctive therapy) when compared with either placebo or no treatment. Side effects were more commonly reported in those patients receiving danazol than for placebo. Authors conclusions Authors conclusions Danazol is effective in treating the symptoms and signs of endometriosis. However, its use is limited by the occurrence of androgenic side effects.
... lire plus sur ce sujet dans un nouvel onglet.... | | | 
|

")
")
 La Naprotechnology et, plus généralement, la médecine restaurative (réparatrice) de la fertilité, est une approche intégrée et systématique de l'infertilité.
La Naprotechnology et, plus généralement, la médecine restaurative (réparatrice) de la fertilité, est une approche intégrée et systématique de l'infertilité.  Douleur
Douleur