| Référence : | | |
| Long versus short course treatment with metformin and clomiphene citrate for ovulation induction in women with PCOS .. cacher .... voir plus ..
Background Background Polycystic ovary syndrome (PCOS) is the most common endocrinopathy among reproductive-aged women. Apart from infertility, women with PCOS often have other endocrine disorders, including insulin resistance, hyperinsulinaemia and hyperandrogenism. Metformin,combined with clomiphene citrate (CC), has been shown to be more effective in ovulation induction when compared with clomiphene citrate alone. The optimal duration for metformin pretreatment before initiation of clomiphene citrate, however, is unknown. Objectives Objectives To determine the effectiveness of short-course (less than four weeks) metformin plus CC versus long-course (four weeks or more) metformin plus CC with regard to ovulation and achievement of pregnancy in infertile women with PCOS. Search methods Search methods We searched the Cochrane Menstrual Disorders and Subfertility Group Trials Register, the Cochrane Central Register of Controlled Trials, MEDLINE, CINAHL, EMBASE and PsycINFO (all from inception to 1 February 2012). Selection criteria Selection criteria Randomised controlled trials comparing short-course (less than four weeks) metformin plus CC versus long-course (four weeks or more) metformin plus CC for ovulation or achievement of pregnancy in infertile women with PCOS. Data collection and analysis Data collection and analysis No trials were found that met the selection criteria. Main results Main results No randomised controlled trials were identified. Authors conclusions Authors conclusions There are insufficient data to determine whether short-course metformin pretreatment is as effective as the conventional long-course metformin pretreatment before initiation of clomiphene citrate for ovulation induction in infertile women with PCOS. A well-designed randomised controlled trial is needed to answer this important clinical question.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Anomalie ou Maladie concernée : | | |
| Syndrome des ovaires polykystiques .. cacher .... voir plus ..
Le syndrome des ovaires polykystiques (SOPK) est un trouble endocrinien (hormonal). Le plus souvent, les symptômes apparaissent pour la première fois à l'adolescence, lors des premières menstruations. Cependant, certaines femmes ne développent pas de symptômes avant le milieu de la vingtaine.
Aucune femme n'a exactement les mêmes symptômes. Les caractéristiques suivantes sont très souvent associées au SOPK, mais toutes ne sont pas visibles chez chaque femme:
Hirsutisme (croissance excessive des cheveux sur le visage, poitrine, abdomen, etc.)
Perte de cheveux (alopécie androgénique, dans un schéma classique de «calvitie masculine»)
Acné
Ovaires polykystiques
Obésité
Infertilité ou fertilité réduite
En outre, les femmes souffrant de SOPK semblent être exposées à un risque accru de développer les problèmes de santé suivants au cours de leur vie:
Résistance à l'insuline
Diabète
Anomalies lipidiques
Apnée obstructive du sommeil
Maladie cardiovasculaire
Cancer de l'endomètre
Étant donné qu'il existe une telle variabilité dans la présentation clinique du SOPK, il n'existe pas d'accord universel parmi les professionnels de la santé sur la manière de mieux définir le syndrome. Ce qui est clair, cependant, c'est que les femmes souffrant de SOPK n'ovulent pas de manière prévisible et produisent également des quantités excessives d'androgènes (testostérone libre et totale, DHEAS).
Les ovaires polykystiques ne sont pas présents chez toutes les femmes diagnostiquées avec SOPK. En outre, de nombreuses femmes ayant des cycles réguliers et un niveau normal de testostérone ont des ovaires kystiques.
Il est important de faire la distinction entre les ovaires polykystiques et le syndrome des ovaires polykystiques.
Les ovaires polykystiques sont souvent, mais pas toujours, observés chez les femmes atteintes de SOPK.
Et environ 20 pour cent des femmes sans anomalies menstruelles ou hormonales ont des ovaires polykystiques.
Le syndrome est donc défini par les anomalies menstruelles et hormonales avec ou sans ovaires polykystiques.
... lire plus sur ce sujet dans un nouvel onglet.... | 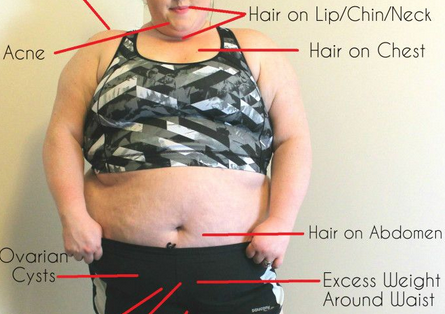 | |
| Référence : | | |
| Correlation of Endometrial Glycodelin Expression and Pregnancy Outcome in Cases with Polycystic Ovary Syndrome Treated with Clomiphene Citrate Plus Metformin: A Controlled Study .. cacher .... voir plus ..
Objective. The purpose of this study was to evaluate the relationship between clomiphene citrate (CC) plus metformin treatment and endometrial glycodelin expression and to then correlate this relationship with pregnancy outcomes. Material and Methods. A total of 30 patients diagnosed with polycystic ovary syndrome (PCOS) according to the Rotterdam criteria constituted our study group. All had been admitted to the gynecology outpatient clinic between June 1, 2011, and January 1, 2012, for infertility treatment. Our control group consisted of 20 patients admitted for routine Pap smear control. They had no history of infertility and were not using contraceptives and they were actively attempting pregnancy. Midluteal progesterone measurement and pipelle endometrial biopsies were performed with both groups. For PCOS patients, metformin treatment was initiated right after the biopsy and CC was added in the second menstrual cycle. Pipelle endometrial biopsies were repeated. Histological dating and immunohistochemistry for glycodelin were performed by a single pathologist who was blinded to the patients clinical data. Result(s). The posttreatment ovulation rate in the study group was 93.3%. No pregnancies were achieved in either group when glycodelin expression was not present, even in the presence of ovulation. When glycodelin expression was high in PCOS group, the pregnancy rate was 60% and all pregnancies ended in live births. In weak expression group, however, three out of four pregnancies ended as early pregnancy losses. Conclusion(s). Endometrial glycodelin expression is an important predictor of pregnancy outcomes in both PCOS and fertile groups.
... lire plus sur ce sujet dans un nouvel onglet.... | | |  |
| Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility .. cacher .... voir plus ..
Background Background Polycystic ovary syndrome (PCOS) is characterised by infrequent or absent ovulation (anovulation), high levels of male hormones (hyperandrogenaemia) and high levels of insulin (hyperinsulinaemia secondary to increased insulin resistance). Hyperinsulinaemia is associated with an increase in cardiovascular risk and the development of diabetes mellitus. Insulin-sensitising agents such as metformin may be effective in treating the features of PCOS, including anovulation. Objectives Objectives To assess the effectiveness of insulin-sensitising drugs in improving reproductive outcomes and metabolic parameters for women with PCOS. Search methods Search methods We searched the Cochrane Menstrual Disorders and Subfertility Group Trials Register (October 2011), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library, 3rd Quarter 2011), CINAHL (October 2011), MEDLINE (January 1966 to October 2011), and EMBASE (January 1985 to October 2011). Selection criteria Selection criteria Randomised controlled trials of insulin sensitising drugs compared with either placebo, no treatment, or an ovulation induction agent for women with PCOS, menstrual disturbance and subfertility. Data collection and analysis Data collection and analysis Two review authors independently assessed studies for inclusion and trial quality, and extracted data. Main results Main results Forty-four trials (3992 women) were included for analysis, 38 of them using metformin and involving 3495 women. There was no evidence that metformin improved live birth rates, whether it was used alone (pooled OR 1.80, 95% CI 0.52 to 6.16, 3 trials, 115 women) or in combination with clomiphene (pooled OR 1.16, 95% CI 0.85 to 1.56, 7 trials, 907 women). However, clinical pregnancy rates were improved for metformin versus placebo (pooled OR 2.31, 95% CI 1.52 to 3.51, 8 trials, 707 women) and for metformin and clomiphene versus clomiphene alone (pooled OR 1.51, 95% CI 1.17 to 1.96, 11 trials, 1208 women). In the studies that compared metformin and clomiphene alone, there was evidence of an improved live birth rate (pooled OR 0.3, 95% CI 0.17 to 0.52, 2 trials, 500 women) and clinical pregnancy rate (pooled OR 0.34, 95% 0.21 to 0.55, 2 trials, 500 women) in the group of obese women who took clomiphene. Metformin was also associated with a significantly higher incidence of gastrointestinal disturbances than placebo (pooled OR 4.27, 95% CI 2.4 to 7.59, 5 trials, 318 women) but no serious adverse effects were reported. Authors conclusions Authors conclusions In agreement with the previous review, metformin was associated with improved clinical pregnancy but there was no evidence that metformin improves live birth rates whether it is used alone or in combination with clomiphene, or when compared with clomiphene. Therefore, the role of metformin in improving reproductive outcomes in women with PCOS appears to be limited.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Effects of Metformin on Spontaneous and Clomiphene-Induced Ovulation in the Polycystic Ovary Syndrome .. cacher .... voir plus ..
Polycystic ovary syndrome, which affects approximately 6 percent of women of reproductive age and is characterized by chronic anovulation and hyperandrogenism,1 is the most common cause of infertility in women in the United States. Insulin resistance with compensatory hyperinsulinemia is a prominent feature of the syndrome2–5 and appears to have a pathophysiologic role in the hyperandrogenism of the disorder. Ovarian androgen production and serum free testosterone concentrations decrease in women with polycystic ovary syndrome when insulin secretion is reduced by drugs such as diazoxide,6 metformin,7–10 and troglitazone.11,12 However, whether such therapy improves ovulatory function is not known. . . .
... lire plus sur ce sujet dans un nouvel onglet.... | | | 
|
| Extended-Release Metformin Does Not Reduce the Clomiphene Citrate Dose Required to Induce Ovulation in Polycystic Ovary Syndrome .. cacher .... voir plus ..
Context: When used for ovulation induction, higher doses of clomiphene may lead to antiestrogenic side effects that reduce fecundity. It has been suggested that metformin in combination with clomiphene can restore ovulation to some clomiphene-resistant anovulators with polycystic ovary syndrome (PCOS)., Objective: Our objective was to determine if cotreatment with extended-release metformin (metformin XR) can lower the threshold dose of clomiphene needed to induce ovulation in women with PCOS., Design: A secondary analysis of data from the National Institute of Child Health and Human Development Cooperative Multicenter Reproductive Medicine Network prospective, double-blind, placebo-controlled multicenter clinical trial, Pregnancy in Polycystic Ovary Syndrome, was performed., Setting: Study volunteers at multiple academic medical centers were included., Participants: Women with PCOS and elevated serum testosterone who were randomized to clomiphene alone or with metformin (n = 209 in each group) were included in the study., Interventions: Clomiphene citrate, 50 mg daily for 5 d, was increased to 100 and 150 mg in subsequent cycles if ovulation was not achieved; half also received metformin XR, 1000 mg twice daily. Treatment was for up to 30 wk or six cycles, or until first pregnancy., Main Outcome Measures: Ovulation was confirmed by a serum progesterone more than or equal to 5 ng/ml, drawn prospectively every 1–2 wk., Results: The overall prevalence of at least one ovulation after clomiphene was 75 and 83% (P = 0.04) for the clomiphene-only and clomiphene plus metformin groups, respectively. Using available data from 314 ovulators, the frequency distribution of the lowest clomiphene dose (50, 100, or 150 mg daily) resulting in ovulation was indistinguishable between the two treatment groups., Conclusion: Metformin XR does not reduce the lowest dose of clomiphene that induces ovulation in women with PCOS., In anovulatory women with polycystic ovary syndrome seeking fertility, metformin does not decrease the clomiphene dose needed to induce ovulation.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| [Using an ovarian drilling by hydrolaparoscopy or recombinant follicle stimulating hormone plus metformin to treat polycystic ovary syndrome: Why a randomized controlled trial fail?] .. cacher .... voir plus ..
OBJECTIVES: To evaluate pregnancy rates after randomized controlled trial (RCT) between ovarian drilling by fertiloscopy or ovarian hyperstimulation+insemination+metformine after clomifène citrate (cc) treatment fails. PATIENTS AND METHODS: Randomized controlled trial with 126 patients in each arm in 9 university centers. After 6-9 months of stimulation by cc, 2 groups were randomized: group 1, ovarian drilling with bipolar energy versus group 2: 3 months treatment by metformine followed by 3 hyperstimulation by FSH+insemination. The success rate was pregnancy rate above 12 weeks. RESULTS: RCT was stopped after the screening of 40 patients. In spite of the low number of patients, the pregnancy rate is significantly higher in medical group 8/16 versus 3/18 (p=0.04). CONCLUSION: The causes of fail of RCT were in relationship with difficulties of inclusion, with absence of final agreement by team included. Moreover, RCT between medical and surgical management is often root of difficulties for patients who decline surgical strategy. However, medical treatment appeared better than drilling in this RCT.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Long versus short course treatment with metformin and clomiphene citrate for ovulation induction in women with PCOS (Review) .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
|
| Evaluating the equivalence of clomiphene citrate with and without metformin in ovulation induction in PCOS patients .. cacher .... voir plus ..
Objective To evaluate the benefit of Metfomin added to Clomiphene Citrate in a primary ovulation induction protocol in PCOS patients Design Prospective randomised controlled study Setting Tygerberg Academic Hospital, Stellenbosch University and the Institute of Reproductive Medicine at Vincent Pallotti Hospital, Cape Town Patients 107 patients presenting with PCOS Study Group A was pre-treated with metformin 850 mg twice a day for at least 6 weeks before clomiphene was added and the metformin was used throughout the study period. Group B received clomiphene without pre-treatment with metformin. In both groups clomiphene was given at a starting dose of 50 mg day 4–8 and increase with increments of 50 mg to a maximum of 150 mg if no response was achieved. Results The ovulation rate achieved in women in the M+C/C arm was 34/52 (65.4%) compared to 36/55 (65.5%) in the C/C arm. The treatment effect ((M+C/C) – C/C) is 0% with 95% confidence interval of −18.1% to 18%. The per protocol ovulation results were 34/42 (81%) in the M+C/C arm compared to 36/48 (75%) in the C/C arm. The ovulation rate difference was 6% with 95% confidence interval −11% to 22%. In a comparison of successful ovulating versus non-ovulating women from the trial the following were significant baseline determinants: lower median weight in the ovulating group (77 kg versus 86 kg, p = .021), lower median bmi (29.0 versus 32.9, p = .009), lower median DHEAS at baseline (4.6 compared to 7.0, p = .049), lower median 17OH-progesterone (2.2 versus 4.6, p = .027) and higher baseline median SHBG ( 37.8 compared to 28.5, p = .036). Conclusion Although identical ovulation rates were observed in both arms equivalence could not be concluded with respect to the specified criteria.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
|

")
")
 Le traitement vise à corriger l'anomalie sous-jacente, dans le but d'optimiser les conditions physiologiques pour la conception in vivo :
Le traitement vise à corriger l'anomalie sous-jacente, dans le but d'optimiser les conditions physiologiques pour la conception in vivo :
 Traitement chirurgical et imagerie interventionnelle de l'infertilité féminine
Traitement chirurgical et imagerie interventionnelle de l'infertilité féminine