| Référence associée : | | |
| Mettler L, Schollmeyer T, Lehmann-Willenbrock E, et al: Accuracy of Laparoscopic Diagnosis of En dometri o sis.
JSLS. 7:15-18, 2003. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Kauppila A, Hartikainen-Sorri A-L, Janne O, Tuimala R, Garvinen PA: Sup pres sion of threatened premature
la bor by administration of cortisol and 17 -hy droxy proges t er one caproate: A com par i son with Ritodrine.
Am J Obstet Gynec 138:404-408, 1980. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Gonadotrophin-releasing hormone analogues for pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is a common gynaecological condition, characterised by the presence of endometrial tissue in sites other than the uterine cavity (excluding adenomyosis) that frequently presents with pain. The gonadotrophin-releasing hormone analogues (GnRHas) comprise one intervention that has been offered for pain relief in pre-menopausal women. GnRHas can be administered intranasally, by subcutaneous, or intramuscular injection. They are thought to result in down regulation of the pituitary and induce a hypogonadotrophic hypogonadal state. Objectives Objectives To determine the effectiveness and safety of GnRHas in the treatment of the painful symptoms associated with endometriosis. Search methods Search methods Electronic searches of the Cochrane Menstrual Disorders and Subfertility Group specialist register, CENTRAL, MEDLINE, EMBASE, PSYCInfo and CINAHL were conducted in April 2010 to identify relevant randomised controlled trials (RCTs). Selection criteria Selection criteria RCTs of GnRHas as treatment for pain associated with endometriosis versus no treatment, placebo, danazol, intra-uterine progestagens, or other GnRHas were included. Trials using add-back therapy, oral contraceptives, surgical intervention, GnRH antagonists or complementary therapies were excluded. Data collection and analysis Data collection and analysis Quality assessment and data extraction were performed independently by two reviewers. The primary outcome was pain relief. Relative risk was used as the measure of effect for dichotomous data. For continuous data, mean differences or standardised mean differences were used. Main results Main results Forty one trials (n=4935 women) were included. The evidence suggested that GnRHas were more effective at symptom relief than no treatment/placebo. There was no statistically significant difference between GnRHas and danazol for dysmenorrhoea RR 0.98 (95%CI 0.92 to 1.04; P = 0.53). This equates to 3 fewer women per 1000 (95%CI 12 to 6) with symptomatic pain relief in the GnRHa group. More adverse events were reported in the GnRHa group. There was a benefit in overall resolution for GnRHas RR1.10 (95%CI 1.01 to 1.21, P=0.03) compared with danazol. There was no statistically significant difference in overall pain between GnRHas and levonorgestrel SMD -0.25 (95%CI -0.60 to 0.10, P=0.46). Evidence was limited on optimal dosage or duration of treatment for GnRHas. No route of administration appeared superior to another. Authors conclusions Authors conclusions GnRHas appear to be more effective at relieving pain associated with endometriosis than no treatment/placebo. There was no evidence of a difference in pain relief between GnRHas and danazol although more adverse events reported in the GnRHa groups. There was no evidence of a difference in pain relief between GnRHas and levonorgestrel and no studies compared GnRHas with analgesics.
... lire plus sur ce sujet dans un nouvel onglet.... | | |  |
| Pentoxifylline for endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is a chronic, recurring condition that occurs during the reproductive years. It is characterized by endometrial tissue developing outside the uterine cavity. This endometrial tissue development is dependent on oestrogen produced primarily by the ovaries and, therefore, traditional management has focused on ovarian suppression. In this review we considered the role of modulation of the immune system as an alternative approach. This is an update of a Cochrane Review previously published in 2009 (Lu 2009). Objectives Objectives To assess the effects of pentoxifylline, which has anti-inflammatory effects, in subfertile, premenopausal women for the management of endometriosis. Search methods Search methods For the first publication of this review we searched the following databases (from inception to December 2008) for trials: Cochrane Menstrual Disorders and Subfertility Group Specialised Register, Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library), MEDLINE, EMBASE, CINAHL, and PsycINFO. In addition, all reference lists of included trials were searched and experts in the field were contacted in an attempt to locate trials. This search was rerun to 23 November 2011, for this update. Selection criteria Selection criteria Randomised controlled trials (RCTs) comparing pentoxifylline with placebo or no treatment, medical treatment, or surgery in subfertile, premenopausal women were included. Data collection and analysis Data collection and analysis Two review authors independently selected trials for inclusion, assessed trial risk of bias, and extracted data using data extraction forms. We contacted study authors for additional information and data. The domains assessed for risk of bias were sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting. Peto odds ratios (OR) were used for reporting dichotomous data with 95% confidence intervals (CI), whilst mean differences (MD) were expressed for continuous data. Statistical heterogeneity was assessed using the I2 statistic. Main results Main results Four trials involving 334 participants were included. One RCT [n=34] showed pentoxifylline had no significant effect on reduction in pain (MD -1.60, 95% CI -3.32 to 0.12). There was no evidence of an increase in clinical pregnancy events in the pentoxifylline group compared with placebo (three RCTs [n=67] OR 1.54, 95% CI 0.89 to 266). One RCT studied recurrence of endometriosis [n=88] (OR 0.88,95% CI 0.27 to 2.84). No trials reported the effects of pentoxifylline on the odds of live birth rate per woman, improvement of endometriosis-related symptoms, or adverse events. Authors conclusions Authors conclusions This review has been updated in 2011. The results of the original review published in 2009 remain unchanged. There is still not enough evidence to support the use of pentoxifylline in the management of premenopausal women with endometriosis in terms of subfertility and relief of pain outcomes.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| [Management of endometriosis ovarian cysts] .. cacher .... voir plus ..
The efficacy of medical treatment as unique treatment for endometrioma is not demonstrated. Operative laparoscopic management is the gold standard for surgical treatment. There is no indication to prescribe preoperatively medical treatment before cystectomy. Post-operative administration of low-dose cyclic oral contraceptive does not significantly affect long-term recurrence rate of endometriosis after surgical treatment. In cases of infertility, management of endometriomas is controversial. Recurrent ovarian surgery is not recommended.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Laparoscopic treatment of pelvic pain associated with minimal and mild endometriosis with use of the Helica Thermal Coagulator .. cacher .... voir plus ..
OBJECTIVE: To investigate the clinical efficacy and safety of Helica Thermal
Coagulator (TC) in the treatment of pelvic pain associated with minimal (stage I)
and mild (stage II) endometriosis.
DESIGN: A clinical observational study.
SETTING: A referral center for laparoscopic treatment of endometriosis.
PATIENT(S): Eighty-one women with pelvic pain symptoms associated with minimal
and mild endometriosis diagnosed at laparoscopy.
INTERVENTION(S): Helica TC to treat endometriotic lesions. The revised American
Fertility Society (rAFS) classification was used to stage endometriosis. Pain
symptoms and patient satisfaction were assessed subjectively at 3 and 6 months
follow-up.
MAIN OUTCOME MEASURE(S): Improvement or relief of pelvic pain symptoms, and
intra- or postoperative complications.
RESULT(S): A total of 79 women completed the study to 6 months follow-up. At 3
months, 59 (74.7%) women reported resolution and satisfactory improvement of
symptoms, whereas 20 (25.3%) women continued to experience painful symptoms. At 6
months, 69 (87.4%) women reported resolution and satisfactory improvement of
symptoms, whereas 9 (11.4%) women reported no changes and 1 (1.2%) woman
experienced worsening symptoms. No significant differences were found between
minimal and mild disease. No side effects or surgical complications occurred.
CONCLUSION(S): Meaningful improvements and relief in clinical symptoms can be
obtained with conservative laparoscopic surgery. Helica TC is a simple,
effective, and safe device for the treatment of pelvic pain in women with stages
I and II endometriosis. This approach requires further evaluation as part of
randomized controlled trials.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Danazol for pelvic pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is defined as the presence of endometrial tissue (stromal and glandular) outside the normal uterine cavity. Conventional medical and surgical treatments for endometriosis aim to remove or decrease the deposits of ectopic endometrium. The observation that hyper androgenic states (an excess of male hormone) induce atrophy of the endometrium has led to the use of androgens in the treatment of endometriosis. Danazol is one of these treatments. The efficacy of danazol is based on its ability to produce a high androgen and low oestrogen environment (a pseudo menopause) which results in atrophy of the endometriotic implants and thus an improvement in painful symptoms. Objectives Objectives To determine the effectiveness of danazol compared to placebo or no treatment in the treatment of the symptoms and signs, other than infertility, of endometriosis in women of reproductive age. Search methods Search methods We searched the Cochrane Menstrual Disorders and Subfertility Group Specialised Register of trials (searched April 2007), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 2, 2007), and MEDLINE (1966 to April 2007). In addition, all reference lists of included trials were searched, and relevant drug companies were contacted for details of unpublished trials. Selection criteria Selection criteria Randomised controlled trials in which danazol (alone or as adjunctive therapy) was compared to placebo or no therapy. Trials which only reported infertility outcomes were excluded. Data collection and analysis Data collection and analysis Only five trials met the inclusion criteria and two authors independently extracted data from these trials. All trials compared danazol to placebo. Three trials used danazol as sole therapy and three trials used danazol as an adjunct to surgery. Although the main outcome was pain improvement other data relating to laparoscopic scores and hormonal parameters were also collected. Main results Main results Treatment with danazol (including adjunctive to surgical therapy) was effective in relieving painful symptoms related to endometriosis when compared to placebo. Laparoscopic scores were improved with danazol treatment (including as adjunctive therapy) when compared with either placebo or no treatment. Side effects were more commonly reported in those patients receiving danazol than for placebo. Authors conclusions Authors conclusions Danazol is effective in treating the symptoms and signs of endometriosis. However, its use is limited by the occurrence of androgenic side effects.
... lire plus sur ce sujet dans un nouvel onglet.... | | | 
|
| Risk factors associated with endometriosis: importance of study population for characterizing disease in the ENDO Study .. cacher .... voir plus ..
OBJECTIVE We sought to identify risk factors for endometriosis and their consistency across study populations in the Endometriosis: Natural History, Diagnosis, and Outcomes (ENDO) Study. STUDY DESIGN In this prospective matched, exposure cohort design, 495 women aged 18–44 years undergoing pelvic surgery (exposed to surgery, operative cohort) were compared to an age- and residence-matched population cohort of 131 women (unexposed to surgery, populationcohort). Endometriosis was diagnosed visually at laparoscopy/laparotomy or by pelvic magnetic resonance imaging in the operative and population cohorts, respectively. Logistic regression estimated the adjusted odds ratios (AORs) and 95% confidence intervals (CIs) for each cohort. RESULTS The incidence of visualized endometriosis was 40% in the operative cohort (11.8% stage 3–4 by revised criteria from the American Society for Reproductive Medicine), and 11% stage 3–4 in the population cohort by magnetic resonance imaging. An infertility history increased the odds of an endometriosis diagnosis in both the operative (AOR, 2.43; 95% CI, 1.57–3.76) and population (AOR, 7.91; 95% CI, 1.69–37.2) cohorts. In the operative cohort only, dysmenorrhea (AOR, 2.46; 95% CI, 1.28–4.72) and pelvic pain (AOR, 3.67; 95% CI, 2.44–5.50) increased the odds of diagnosis, while gravidity (AOR, 0.49; 95% CI, 0.32–0.75), parity (AOR, 0.42; 95% CI, 0.28–0.64), and body mass index (AOR, 0.95; 95% CI, 0.93–0.98) decreased the odds of diagnosis. In all sensitivity analyses for different diagnostic subgroups, infertility history remained a strong risk factor. CONCLUSION An infertility history was a consistent risk factor for endometriosis in both the operative and population cohorts of the ENDO Study. Additionally, identified risk factors for endometriosis vary based upon cohort selection and diagnostic accuracy. Finally, endometriosis in the population may be more common than recognized.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
|
| Progestagens and anti-progestagens for pain associated with endometriosis .. cacher .... voir plus ..
Background Background Endometriosis is a chronic inflammatory condition defined by the presence of glands and stroma outside the uterine cavity. It occurs in 7% to 10% of all women of reproductive age and may present as pain or infertility. The pelvic pain may be in the form of dysmenorrhoea, dyspareunia or pelvic pain. Initially a combination of estrogens and progestagens was used to create a pseudopregnancy and alleviate the symptoms associated with endometriosis. Progestagens alone or anti-progestagens have been considered as alternatives because they are inexpensive and may have a better side effect profile than other choices. Objectives Objectives To determine the effectiveness of both the progestagens and anti-progestagens in the treatment of painful symptoms ascribed to the diagnosis of endometriosis. Search methods Search methods We used the search strategy of the Menstrual Disorders and Subfertility Group to identify all publications which described or might have described randomised controlled trials (RCTs) of any progestagen or any anti-progestagen in the treatment of symptomatic endometriosis. We updated the review in 2011. Selection criteria Selection criteria We considered only RCTs which compared the use of progestagens and anti-progestagens with other interventions, placebo or no treatment for the alleviation of symptomatic endometriosis. Data collection and analysis Data collection and analysis We have added six new studies, bringing the total of included studies to 13 in the update of this review. The six newly included studies evaluated progestagens (comparisons with placebo, danazol, oral or subdermal contraceptive, oral contraceptive pill and danazol, gonadotrophin-releasing hormone (GnRH) analogue and other drugs). The remaining studies compared the anti-progestagen gestrinone with danazol, GnRH analogues or itself. Main results Main results The progestagen medroxyprogesterone acetate (100 mg daily) appeared to be more effective at reducing all symptoms up to 12 months of follow-up (MD -0.70, 95% CI -8.61 to -5.39; P < 0.00001) compared with placebo. There was evidence of significantly more cases of acne (six versus one) and oedema (11 versus one) in the medroxyprogesterone acetate group compared with placebo. There was no evidence of a difference in objective efficacy between dydrogesterone and placebo. There was no evidence of a benefit with depot administration of progestagens versus other treatments (low dose oral contraceptive or leuprolide acetate) for reduced symptoms. The depot progestagen group experienced significantly more adverse effects. There was no overall evidence of a benefit of oral progestagens over other medical treatment at six months of follow-up for self-reported efficacy. Amenorrhoea and bleeding were more frequently reported in the progestagen group compared with other treatment groups. There was no evidence of a benefit of anti-progestagens (gestrinone) compared with danazol. GnRH analogue (leuprorelin) was found to significantly improve dysmenorrhoea compared with gestrinone (MD 0.82, 95% CI 0.15 to 1.49; P = 0.02) although it was also associated with increased hot flushes (OR 0.20, 95% CI 0.06 to -0.63; P = 0.006). Authors conclusions Authors conclusions There is only limited evidence to support the use of progestagens and anti-progestagens for pain associated with endometriosis.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Pain typology and incident endometriosis .. cacher .... voir plus ..
STUDY QUESTION What are the pain characteristics among women, with no prior endometriosis diagnosis, undergoing laparoscopy or laparotomy regardless of clinical indication? SUMMARY ANSWER Women with surgically visualized endometriosis reported the highest chronic/cyclic pain and significantly greater dyspareunia, dysmenorrhea, and dyschezia compared with women with other gynecologic pathology (including uterine fibroids, pelvic adhesions, benign ovarian cysts, neoplasms and congenital Müllerian anomalies) or a normal pelvis. WHAT IS KNOWN ALREADY Prior research has shown that various treatments for pain associated with endometriosis can be effective, making identification of specific pain characteristics in relation to endometriosis necessary for informing disease diagnosis and management. STUDY DESIGN, SIZE, DURATION The study population for these analyses includes the ENDO Study (2007–2009) operative cohort: 473 women, ages 18–44 years, who underwent a diagnostic and/or therapeutic laparoscopy or laparotomy at one of 14 surgical centers located in Salt Lake City, UT or San Francisco, CA. Women with a history of surgically confirmed endometriosis were excluded. PARTICIPANTS/MATERIALS, SETTING AND METHODS Endometriosis was defined as surgically visualized disease; staging was based on revised American Society for Reproductive Medicine (rASRM) criteria. All women completed a computer-assisted personal interview at baseline specifying 17 types of pain (rating severity via 11-point visual analog scale) and identifying any of 35 perineal and 60 full-body front and 60 full-body back sites for which they experienced pain in the last 6 months. MAIN RESULTS AND THE ROLE OF CHANCE There was a high prevalence (≥30%) of chronic and cyclic pelvic pain reported by the entire study cohort regardless of post-operative diagnosis. However, women with a post-operative endometriosis diagnosis, compared with women diagnosed with other gynecologic disorders or a normal pelvis, reported more cyclic pelvic pain (49.5% versus 31.0% and 33.1%, P < 0.001). Additionally, women with endometriosis compared with women with a normal pelvis experienced more chronic pain (44.2 versus 30.2%, P = 0.04). Deep pain with intercourse, cramping with periods, and pain with bowel elimination were much more likely reported in women with versus without endometriosis (all P < 0.002). A higher percentage of women diagnosed with endometriosis compared with women with a normal pelvis reported vaginal (22.6 versus 10.3%, P < 0.01), right labial (18.4 versus 8.1%, P < 0.05) and left labial pain (15.3 versus 3.7%, P < 0.01) along with pain in the right/left hypogastric and umbilical abdominopelvic regions (P < 0.05 for all). Among women with endometriosis, no clear and consistent patterns emerged regarding pain characteristics and endometriosis staging or anatomic location. LIMITATIONS, REASONS FOR CAUTION Interpretation of our findings requires caution given that we were limited in our assessment of pain characteristics by endometriosis staging and anatomic location due to the majority of women having minimal (stage I) disease (56%) and lesions in peritoneum-only location (51%). Significance tests for pain topology related to gynecologic pathology were not corrected for multiple comparisons. WIDER IMPLICATIONS OF THE FINDINGS Results of our research suggest that while women with endometriosis appear to have higher pelvic pain, particularly dyspareunia, dysmenorrhea, dyschezia and pain in the vaginal and abdominopelvic area than women with other gynecologic disorders or a normal pelvis, pelvic pain is commonly reported among women undergoing laparoscopy, even among women with no identified gynecologic pathology. Future research should explore causes of pelvic pain among women who seek out gynecologic care but with no apparent gynecologic pathology. Given our and other s research showing little correlation between pelvic pain and rASRM staging among women with endometriosis, further development and use of a classification system that can better predict outcomes for endometriosis patients with pelvic pain for both surgical and nonsurgical treatment is needed. STUDY FUNDING/COMPETING INTERESTS Supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development (contracts NO1-DK-6-3428, NO1-DK-6-3427, and 10001406-02). The authors have no potential competing interests.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Interrater and intrarater reliability in the diagnosis and staging of endometriosis .. cacher .... voir plus ..
OBJECTIVE: To estimate the interrater and intrarater reliability of endometriosis diagnosis and severity of disease among gynecologic surgeons viewing operative digital images. METHODS: The study population comprised a random sample (n=148 [36%]) of women who participated in the Endometriosis: Natural History, Diagnosis and Outcomes study. Four academic expert and four local, specialized expert surgeons reviewed the images, diagnosed the presence or absence of endometriosis for each woman, and rated severity using the revised American Society for Reproductive Medicine (ASRM) criteria. Interrater-level and intrarater-level agreement were calculated for both endometriosis diagnosis and staging. RESULTS: The interrater reliability for endometriosis diagnosis among the eight surgeons was substantial: Fleiss κ=0.69 (95% confidence interval [CI] 0.64-0.74). Surgeons agreed on revised ASRM endometriosis staging criteria after experienced assessment in a majority of cases (mean 61%, range 52-75%) with moderate interrater reliability: Fleiss κ=0.44 (95% CI 0.41-0.47). The intrarater reliability for experienced assessment compared with computer-assisted revised ASRM staging was almost perfect (mean weighted κ=0.95, range 0.89-0.99). CONCLUSION: Substantial reliability was found for revised ASRM endometriosis diagnosis, whereas moderate reliability was observed for staging. Almost perfect reliability was observed for surgeons rating of disease severity compared with computerized-assisted, checklist-based staging. Findings suggest that reliability in endometriosis diagnosis is not greatly altered by location or composition of surgeons, supporting the conduct of multisite studies or compilation of endometriosis data across clinical centers. Although surgeons appear to be skilled at assessing endometriosis stage intuitively, how staging of disease burden correlates with clinical outcomes remains to be developed.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Johnson JWC, Austin KL, Jones GS, Davis GH, King TM: Effi cacy of 17 -hydroxyprogesterone caproate
in the pre ven tion of pre ma ture labor. N Engl J Med 293:675-680, 1975. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Perfluorochemicals and Endometriosis The ENDO Study .. cacher .... voir plus ..
Background: Environmental chemicals may be associated with endometriosis. No published research has focused on the possible role of perfluorochemicals (PFCs) despite their widespread presence in human tissues. Methods: We formulated two samples. The first was an operative sample comprising 495 women aged 18–44 years scheduled for laparoscopy/laparotomy at one of 14 participating clinical sites in the Salt Lake City or San Francisco area, 2007–2009. The second was a population-based sample comprising 131 women matched to the operative sample on age and residence within a 50-mile radius of participating clinics. Interviews and anthropometric assessments were conducted at enrollment, along with blood collection for the analysis of nine PFCs, which were quantified using liquid chromatography-tandem mass spectrometry. Endometriosis was defined based on surgical visualization (in the operative sample) or magnetic resonance imaging (in the population sample). Using logistic regression, we estimated odds ratios (ORs) and 95% confidence intervals (CIs) for each PFC (log-transformed), adjusting for age and body mass index, and then parity. Results: Serum perfluorooctanoic acid (PFOA; OR = 1.89 [95% CI = 1.17–3.06]) and perfluorononanoic acid (2.20 [1.02–4.75]) were associated with endometriosis in the operative sample; findings were moderately attenuated with parity adjustment (1.62 [0.99–2.66] and 1.99 [0.91–4.33], respectively). Perfluorooctane sulfonic acid (1.86 [1.05–3.30]) and PFOA (2.58 [1.18–5.64]) increased the odds for moderate/severe endometriosis, although the odds were similarly attenuated with parity adjustment (OR = 1.50 and 1.86, respectively). Conclusions: Select PFCs were associated with an endometriosis diagnosis. These associations await corroboration.
... lire plus sur ce sujet dans un nouvel onglet.... | | | |
| Buchweitz O, Poel T, Diedrich K, et al: The Diagnostic Dilemma of Minimal and Mild Endometriosis Under
Rou tine Con di tions. J Am Assoc Gynecol Laparosc 10:85-89, 2003. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| L'endométriose est fortement associée à l'infertilité.
D’Hooghe TM, Debrock S, Hill JA, et al: Endometriosis and Subfertility: Is the Relationship Resolved? Sem
Reprod Med 21:243-253, 2003. .. cacher .... voir plus ..
The endometriosis has an adverse effect on fertility by being strongly associated with infertility.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| L'endométriose est associée à un risque plus élevée de fausses couches.
Naples JD, Batt RE, Sadijh H: Spon ta ne ous Abortion Rate in Patients with En dometri o sis. Obstet Gynecol
57:509-512, 1981. .. cacher .... voir plus ..
The endometriosis is associated with a higher risk of spontaneous abortion
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Groll M: Endometriosis and Spon ta ne ous Abortion. Fertil Steril 41:933-935, 1984. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Anomalie ou Maladie concernée : | | |
| Endométriose .. cacher .... voir plus ..
L'endométriose désigne une affection se caractérisant par une implantation du tissu endométrial dans des localisations autres que celle de la muqueuse utérine.
L'endométriose est retrouvée de manière prédominante au niveau du colon sigmoïde, du rectum antérieur, de l'iléon terminal et du caecum.
Ce qui demeure frappant est la quasi absence de développement du tissu endométrial dans les trompes de Fallope. De nombreuses autres localisations peuvent être retrouvées.
Considérée comme une tumeur bénigne, il a été toutefois rapporté des cas de malignité.
L'endométriose est une maladie chirurgicale. Le traitement médical (danazol, leucoprolide, contraceptifs oraux) ne permet qu'un soulagement temporaire de la douleur, mais aucun traitement médical n'a été efficace dans le traitement de l'endométriose. Seule une prise en charge chirurgicale est efficace et permet d'éradiquer la maladie.
... lire plus sur ce sujet dans un nouvel onglet.... | 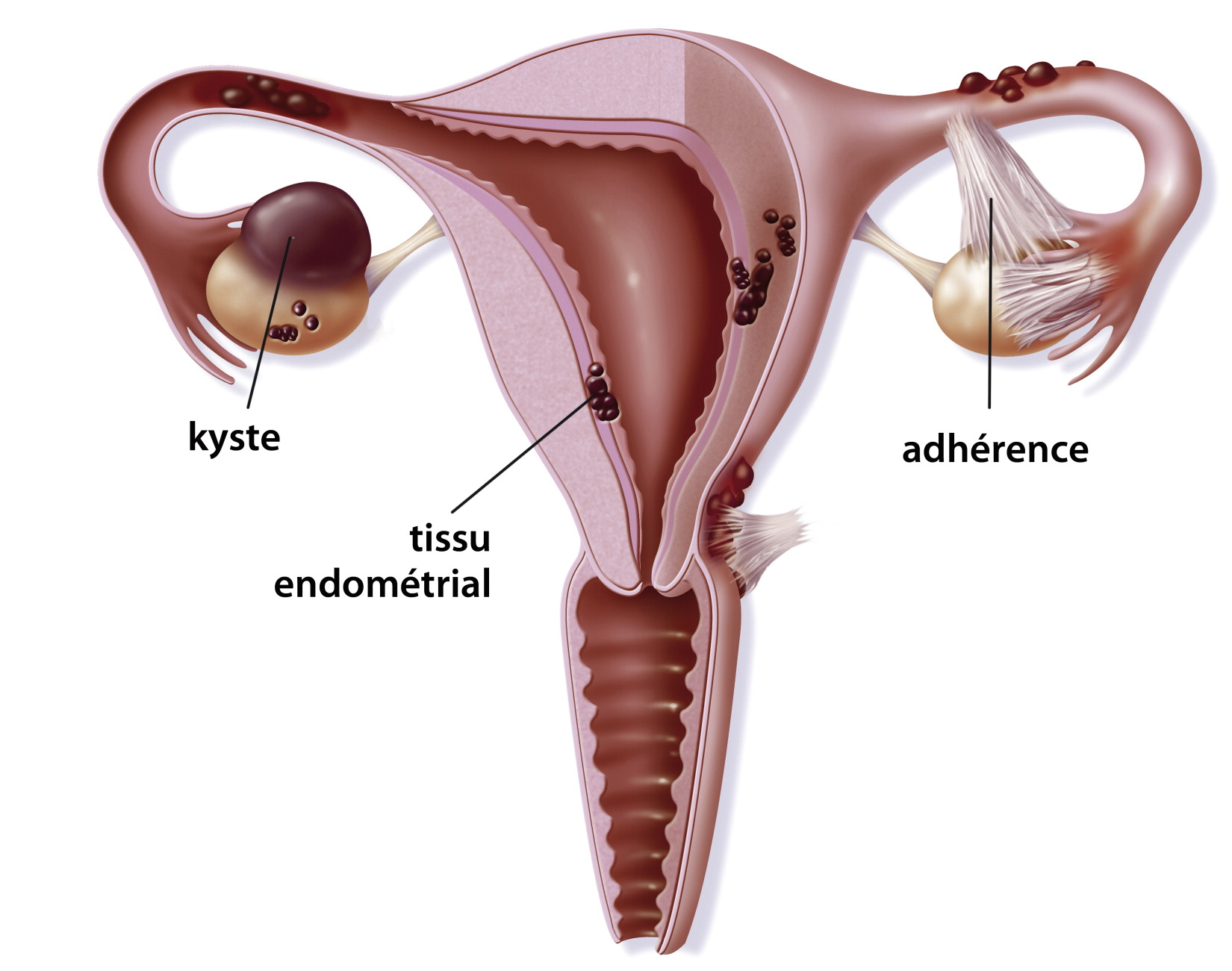 | |
| Référence associée : | | |
| Pittaway DE, Vernon C, Fayez JA: Spon ta ne ous Abortions in Women with En dometri o sis. Fertil Steril
50:711-715, 1988. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Olive DL, Franklin RR, Gratkins LV: The Association Be tween Endometriosis and Spontaneous Abor tion:
A Ret ro spect of Clinical Study. J Reprod Med 27:333-338, 1982. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Haney AF, Muscato JJ, Weinberg JB: Peri to neal Fluid Cell Populations in In fer til i ty Patients. Fertil Steril
35:696-697, 1981 .. cacher .... voir plus ..
The peritoneal fluid in women with endometriosis increases in volume
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Morcos RN, Gibbons WE: Effect of Peri to neal Fluid on In Vitro Cleavage of 2-Cell Mouse Embryos: Possible
Role in Infertility Associated with En dometri o sis. Fertil Steril 44:678,1985. .. cacher .... voir plus ..
In peritoneal fluid from infertile women who have endometriosis, it has been found that it is toxic to the growth and developpement of mouse embryos when compared to the fluid from normal women and infertile women without endometriosis.
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Gerrity M, Rinehart JS, Shapiro SS: The Effect of Human Peritoneal Fluid on Embryonic Development.
Annual Meet ing of the American Fertility So ci ety. Abstract #58, 1985. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| L'infertilité serait litée à une qualité médiocre des embryons dérivant d'oocytes altérées résultants d'un dysfonctionnement des ovaires
Garrido N, Pellicer A, Remohi J, et al: Uterine and Ovarian Function in En dometri o sis. Sem Reprod Med
21:183-191, 2003. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |
| Une méta-analyse a montré de manière convaincante la supériorité du traitement chirurgical sur le traitement médical des cas d'endométriose associée à l'infertilité.
Kim AH, Adamson GD: Does Therapy for Minimal/Mild Endometriosis En hance Conception? Inf Reprod
Med Clin North Am 8:623-637, 1997. .. cacher .... voir plus ..
... lire plus sur ce sujet dans un nouvel onglet.... | | |

")
")
 Médecine par les plantes, la nutrition et l'activité, mode de vie, acupuncture
Médecine par les plantes, la nutrition et l'activité, mode de vie, acupuncture